Obesity
A clinical reference for UK primary care
Last reviewed 2 May 2026 · Next review August 2026
Obesity is now classified as a chronic relapsing condition. Management has shifted from short-term lifestyle interventions toward sustained long-term care, with pharmacotherapy and structured weight management services taking a more prominent role.1,2
Around 26% of adults in England live with obesity (BMI ≥30), and a further 38% are overweight.4
Prevalence is highest in the most deprived areas, where access to specialist weight management services is often most constrained.4
Recent in obesity
2 Apr 2026
GLP-1 for Alzheimer's? EVOKE trial says no

13 Mar 2026
GLP-1 Receptor Agonists: Mechanism of Action
22 Feb 2026
MHRA Safety Update: Semaglutide and the Risk of Rare Vision Loss
5 Feb 2026
The GLP-1 revolution: the good, the bad and the ugly
4 May 2026
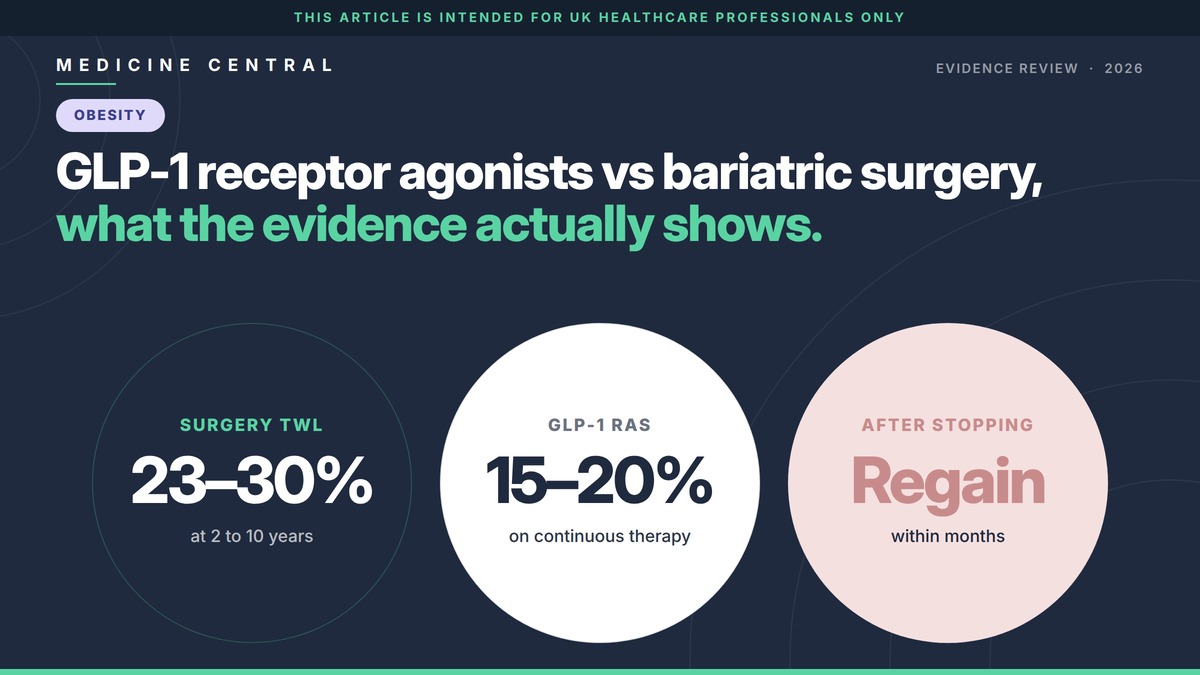
GLP-1 receptor agonists vs bariatric surgery, what the evidence actually shows.
BMI classification and waist measurement
WHO BMI categories are the standard starting point. Adjusted thresholds apply for South Asian, Chinese, other Asian, Black African and African Caribbean populations.1,6
Validated tools used in primary care
CARDIOMETABOLIC
QRISK3, HbA1c, lipids, BP
Cardiovascular and metabolic risk assessment as part of the annual review. QRISK3 remains the standard CV risk tool in UK primary care.9
HEPATIC
Liver fibrosis assessment
Non-invasive screening for advanced fibrosis in non-alcoholic fatty liver disease (now widely termed MASLD). NICE NG49 recommends ELF as first-line; FIB-4 is widely used in primary care per BSG guidance.10
SLEEP
STOP-BANG questionnaire
Validated screening tool for obstructive sleep apnoea risk. Particularly relevant in BMI ≥35 with daytime symptoms.11
FUNCTIONAL STAGING
Edmonton Obesity Staging System
Captures functional, mental and metabolic impact beyond BMI alone. Increasingly referenced in tier 3 assessment.8
The four tiers of weight management
NHS weight management services are commissioned in four tiers of escalating intensity.12
NHS England: Adult Weight Management Services
Tier definitions and commissioning guidance
Universal
Public health interventions and brief advice in primary care
Community
Structured 12-week lifestyle programmes
Refer when
BMI ≥30, or ≥27.5 in higher-risk ethnicities. Local commissioning varies, with some areas restricting referral to those with comorbidities.1,12
Specialist
Multidisciplinary consultant-led service
Refer when
BMI ≥40, or ≥35 with comorbidities, after tier 2 intervention has been considered. Lower thresholds apply in higher-risk ethnicities.1,12
Surgical
Bariatric surgery and specialist pharmacotherapy
Refer when
BMI ≥40, or ≥35 with significant comorbidities, following tier 3 input. Direct referral routes vary by ICB.1
Also consider referring
Consider with rapid unexplained weight gain, suspected Cushingoid features, untreated severe hypothyroidism, or pituitary symptoms.1
Where binge eating disorder, bulimia nervosa or other eating disorder is identified. Refer per NG69 and consider before any weight management intervention.13
Find all NICE updates relevant to primary care
View NICE GuidelinesThis disease hub is intended for UK Healthcare Professionals only. Content reports established clinical knowledge and current NICE guidance. It is not a substitute for clinical judgment or for the original guidelines. Last reviewed 28 April 2026.
References
All sources verified at last review. Where primary literature is cited, original peer-reviewed publications are linked.
- 1.National Institute for Health and Care Excellence. Obesity: identification, assessment and management. Clinical guideline CG189.
- 3.Bray GA, Kim KK, Wilding JPH; World Obesity Federation. Obesity: a chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes Rev. 2017;18(7):715-723.
- 5.Office for Health Improvement and Disparities. Obesity profile: short statistical commentary.
- 7.National Institute for Health and Care Excellence. Cardiovascular disease: risk assessment and reduction, including lipid modification. NICE guideline NG238.
- 9.Hippisley-Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ. 2017;357:j2099.
- 11.Chung F, Yegneswaran B, Liao P, et al. STOP questionnaire: a tool to screen patients for obstructive sleep apnea. Anesthesiology. 2008;108(5):812-821.
- 13.National Institute for Health and Care Excellence. Eating disorders: recognition and treatment. NICE guideline NG69.
- 2.World Health Organization. Obesity and overweight fact sheet.
- 4.NHS Digital. Health Survey for England, 2022 Part 2: Adult overweight and obesity.
- 6.National Institute for Health and Care Excellence. BMI: preventing ill health and premature death in black, Asian and other minority ethnic groups. Public health guideline PH46.
- 8.Sharma AM, Kushner RF. A proposed clinical staging system for obesity. Int J Obes (Lond). 2009;33(3):289-295.
- 10.National Institute for Health and Care Excellence. Non-alcoholic fatty liver disease (NAFLD): assessment and management. NICE guideline NG49.
- 12.Office for Health Improvement and Disparities. Weight management: guidance for commissioners and providers.