Chronic Kidney Disease
A clinical reference for UK primary care
Last reviewed 2 May 2026 · Next review July 2026
CKD management has shifted in recent years. NG203 reframed referral around risk rather than eGFR alone, and SGLT2 inhibitors are now incorporated into NICE technology appraisals across CKD with and without diabetes.1
Around 7.2 million people in the UK live with CKD, but more than a million remain undiagnosed.2
Most CKD is managed in primary care, with referral reserved for those at higher risk of progression to kidney failure or with specific clinical features warranting specialist input.1
Recent in chronic kidney disease
28 Apr 2026
NG28 NICE GUIDELINES: The Flozin-First Era, and 810,000 More GLP-1 Patients
2 Apr 2026
SGLT2 trial watch
2 Apr 2026
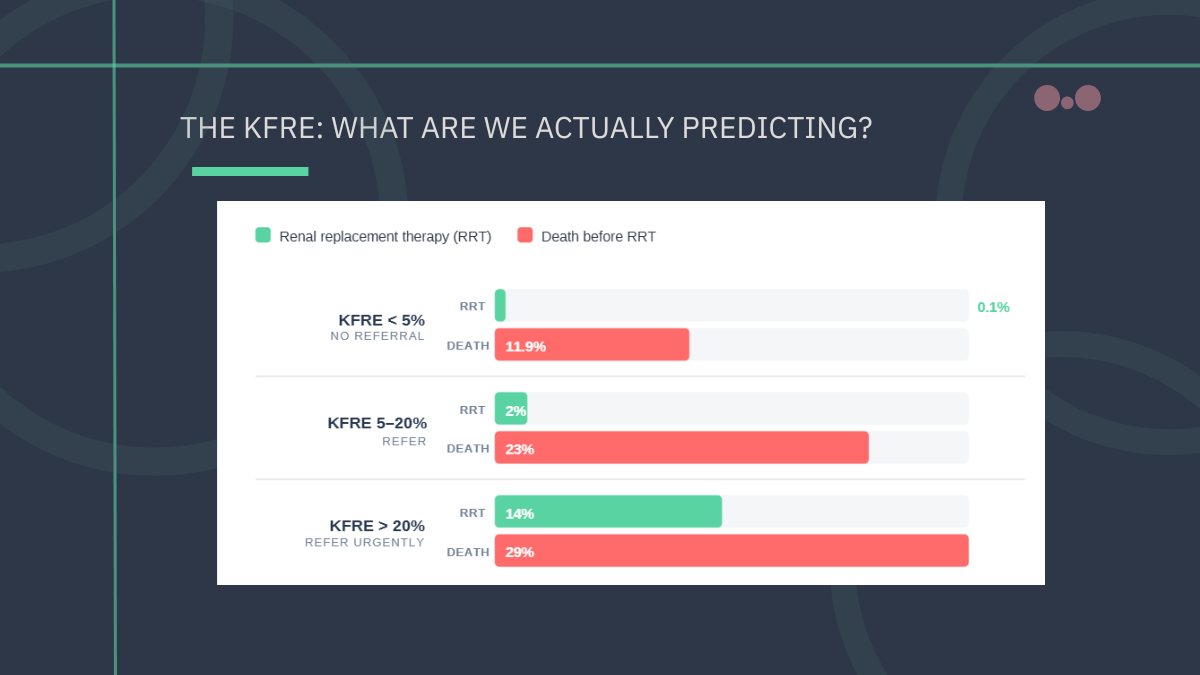
The Kidney Failure Risk Equation: who should we refer?

2 Apr 2026
Falling through the GAAP: when patients diagnose themselves
11 Mar 2026
SGLT2i vs GLP-1 RA: which one offers more kidney protection?
Diagnostic criteria
CKD is defined by abnormalities of kidney structure or function present for more than 3 months. Two main markers: eGFR and albuminuria.1
Reduced eGFR
< 60 mL/min/1.73m²
Sustained for more than 3 months. NG203 specifies eGFR should not be adjusted by an ethnicity factor.1
Albuminuria
ACR ≥3 mg/mmol
Confirm on early morning sample. Repeat is not needed if initial ACR is 70 mg/mmol or more.1
Other markers of kidney damage
Structural or pathological
Haematuria of renal origin, electrolyte abnormalities, structural changes on imaging, or biopsy-proven disease.1
Confirming the diagnosis
A single abnormal eGFR is not sufficient. Confirm with a repeat sample within 2 weeks if eGFR < 60 for the first time, then sustained reduction over 3 months to confirm chronicity. Always consider acute kidney injury before labelling as CKD.1
Risk and monitoring in primary care
Kidney Failure Progression
Cardiovascular
Accelerated Progression
eGFR drop and category change
Defined by NG203 as a sustained decrease in eGFR of 25% or more and a change in GFR category within 12 months, or a sustained decrease of 15 mL/min/1.73m² per year.1
CKD categories: eGFR and ACR
CKD is described by two parameters: eGFR category (G1-G5) and albuminuria category (A1-A3). Classification adopted from KDIGO.1
eGFR Categories
Albuminuria Categories (ACR)
Referral pathways
Per NG203: 5-year KFRE >5%, ACR ≥70 mg/mmol (unless diabetes-related and appropriately treated), ACR >30 mg/mmol with haematuria, accelerated eGFR decline, hypertension uncontrolled despite four agents, or suspected genetic cause.1
Suspected AKI, hyperkalaemia ≥6.5 mmol/L (per UK Kidney Association), or features suggesting acute glomerulonephritis.1,7
Visible haematuria in adults aged 45 and over without UTI, or persisting after treatment, per NG12. Suspected obstruction on imaging.8
Where CKD coexists with diabetes and management is becoming complex. NG28 covers SGLT2 inhibitor positioning in this group.9
Find all NICE updates relevant to primary care
View NICE GuidelinesThis disease hub is intended for UK Healthcare Professionals only. Content reports established clinical knowledge and current NICE guidance. It is not a substitute for clinical judgment or for the original guidelines. Last reviewed 3 May 2026.
References
All sources verified at last review. Where primary literature is cited, original peer-reviewed publications are linked.
- 1.National Institute for Health and Care Excellence. Chronic kidney disease: assessment and management. NICE guideline NG203. Published August 2021, last reviewed September 2024.
- 3.Major RW, Shepherd D, Medcalf JF, Xu G, Gray LJ, Brunskill NJ. The Kidney Failure Risk Equation for prediction of end stage renal disease in UK primary care: An external validation and clinical impact projection cohort study. PLOS Med. 2019;16(11):e1002955.
- 5.Hippisley-Cox J, Coupland C, Brindle P. Development and validation of QRISK3 risk prediction algorithms to estimate future risk of cardiovascular disease: prospective cohort study. BMJ. 2017;357:j2099.
- 7.Alfonzo A, Harrison A, Baines R, Chu A, Mann S, MacRury M; UK Kidney Association. Clinical Practice Guidelines: Treatment of Acute Hyperkalaemia in Adults. UK Kidney Association; 2023.
- 9.National Institute for Health and Care Excellence. Type 2 diabetes in adults: management. NICE guideline NG28.
- 2.Kidney Care UK. Facts about kidneys.
- 4.National Institute for Health and Care Excellence. Cardiovascular disease: risk assessment and reduction, including lipid modification. NICE guideline NG238.
- 6.Mikhail A, Brown C, Williams JA, et al; UK Kidney Association. UK Kidney Association Clinical Practice Guideline: Update of Anaemia of Chronic Kidney Disease. UK Kidney Association; 2024.
- 8.National Institute for Health and Care Excellence. Suspected cancer: recognition and referral. NICE guideline NG12.